ABSTRACTS SELECTED IN NAPCON 2013 CHENNAI
TUBERCULAR ELBOW JOINT SINOVITIS COEXISTING WITH INGUINAL LYMPHADENOPATHY : A RARE CASE PRESENTATION
Author 1 :DR..Kamal deep
Author 2 :Dr.AP Kansal
Author 3 :Dr. Naresh Kumar
Author 4 : Dr. Kalpesh Patel
INTRODUCTION: Tuberculous arthritis and tenosynovitis of the elbow joint are relatively rare as compared with other joints. Making an early diagnosis is often difficult, and treatment is therefore frequently delayed in clinical practice. Synovial thickening of the radio-humeral segment of the articulation can be normally felt, particularly if the synovium is involved.
CASE REPORT: A 28 year old male presented to us with chief complaints of pain and discharge from sinus in the left elbow joint , fever on and off from 8 month. On examination, the patient had swelling at level of left elbow with discharging sinus on the back of elbow. The patient was not able to flex the arm due to spasm of muscles. The patient also had swelling in inguinal area about 5x5 cm, soft in consistency. Pus around 5ml aspirated from inguinal swelling. AFB was positive in pus from both sites. There was no evidence of any other organ involvement. X-ray of elbow joint show that bones were not involved. The patient started on RNTCP Cat I to which he responded well.
DISCUSSION: Tuberculosis of the elbow, like pyogenic arthritis, is characteristically a mono-articular disease, although multifocal osteoarticular tuberculosis does occur. The diagnosis depends on the recognition of M. tuberculosis on either histologic study or culture, or, ideally, both. Juxta-articular osteoporosis and swelling of soft tissue are the earliest roentgenographic changes observed when involvement of a joint occurs. A high level of clinical vigilance is needed to make an early diagnosis of tuberculous synovitis.
Author 1 :DR..Kamal deep
Author 2 :Dr.AP Kansal
Author 3 :Dr. Naresh Kumar
Author 4 : Dr. Kalpesh Patel
INTRODUCTION: Tuberculous arthritis and tenosynovitis of the elbow joint are relatively rare as compared with other joints. Making an early diagnosis is often difficult, and treatment is therefore frequently delayed in clinical practice. Synovial thickening of the radio-humeral segment of the articulation can be normally felt, particularly if the synovium is involved.
CASE REPORT: A 28 year old male presented to us with chief complaints of pain and discharge from sinus in the left elbow joint , fever on and off from 8 month. On examination, the patient had swelling at level of left elbow with discharging sinus on the back of elbow. The patient was not able to flex the arm due to spasm of muscles. The patient also had swelling in inguinal area about 5x5 cm, soft in consistency. Pus around 5ml aspirated from inguinal swelling. AFB was positive in pus from both sites. There was no evidence of any other organ involvement. X-ray of elbow joint show that bones were not involved. The patient started on RNTCP Cat I to which he responded well.
DISCUSSION: Tuberculosis of the elbow, like pyogenic arthritis, is characteristically a mono-articular disease, although multifocal osteoarticular tuberculosis does occur. The diagnosis depends on the recognition of M. tuberculosis on either histologic study or culture, or, ideally, both. Juxta-articular osteoporosis and swelling of soft tissue are the earliest roentgenographic changes observed when involvement of a joint occurs. A high level of clinical vigilance is needed to make an early diagnosis of tuberculous synovitis.
PULMONARY NOCARDIASIS PRESENTING AS UNILATERAL MASSIVE EFFUSION IN IMMUNOCOMPETANT HOST: AN UNUSAL HOST RESPONSE
Author 1 :Dr.AP Kansal
Author 2 :Dr.Gopal Chawla
Author 3 :Dr.Kamal Deep
Author 4 : Dr. Naresh Kumar
INTRODUCTION: Pulmonary nocardiosis (PN) is an infrequent and severe infection due to Nocardia spp., microorganisms that may behave both as opportunists and as primary pathogens. The risk of pulmonary or disseminated disease is more in persons with deficient cell mediated immunity.
Case report: A 38 year old manual labourer presented with chief complaints of progressive breathlessness which increased from grade I to grade III over a period of one month, chest pain and mild dry cough for last 10 days. CXR revealed homogenous opacity left side pushing mediastinal structures to the other side. CECT chest showed left sided massive effusion with complete collapse of ipsilateral lung along with mediastinal lymphadenopathy. Intercostal chest tube drainage was done and around 6l of fluid drained over a period of 6 days. The patient was non reactive to HIV, non-diabetic and was not on any other medication and there was no other finding suggestive of immunosupression. LBC(liquid based cytology) and MGG(May Gruenwald giemsa) smear of pleural fluid showed features those of pleural effusion due to nocardiosis. The pleural fluid grew Nocardia after 2weeks of culture on Sabourauds dextrose agar at 37 °C. Patient started on trimethoprim-sulfamethaxazole and oral steroids. The patient responded well to treatment.
DISCUSSION: Nocardiosis is an acute, sub-acute or chronic infectious disease that occurs in cutaneous, pulmonary and disseminated forms. Pulmonary nocardiasis is usually in form of pneumonitis and is mostly seen in immunocompromised patients. Pulmonary nocardiasis in form of massive unilateral pleural effusion in immunocompetant host without underlying pneumonitis is a rare condition.
Author 1 :Dr.AP Kansal
Author 2 :Dr.Gopal Chawla
Author 3 :Dr.Kamal Deep
Author 4 : Dr. Naresh Kumar
INTRODUCTION: Pulmonary nocardiosis (PN) is an infrequent and severe infection due to Nocardia spp., microorganisms that may behave both as opportunists and as primary pathogens. The risk of pulmonary or disseminated disease is more in persons with deficient cell mediated immunity.
Case report: A 38 year old manual labourer presented with chief complaints of progressive breathlessness which increased from grade I to grade III over a period of one month, chest pain and mild dry cough for last 10 days. CXR revealed homogenous opacity left side pushing mediastinal structures to the other side. CECT chest showed left sided massive effusion with complete collapse of ipsilateral lung along with mediastinal lymphadenopathy. Intercostal chest tube drainage was done and around 6l of fluid drained over a period of 6 days. The patient was non reactive to HIV, non-diabetic and was not on any other medication and there was no other finding suggestive of immunosupression. LBC(liquid based cytology) and MGG(May Gruenwald giemsa) smear of pleural fluid showed features those of pleural effusion due to nocardiosis. The pleural fluid grew Nocardia after 2weeks of culture on Sabourauds dextrose agar at 37 °C. Patient started on trimethoprim-sulfamethaxazole and oral steroids. The patient responded well to treatment.
DISCUSSION: Nocardiosis is an acute, sub-acute or chronic infectious disease that occurs in cutaneous, pulmonary and disseminated forms. Pulmonary nocardiasis is usually in form of pneumonitis and is mostly seen in immunocompromised patients. Pulmonary nocardiasis in form of massive unilateral pleural effusion in immunocompetant host without underlying pneumonitis is a rare condition.
COUGH MAKING GROUND FOR SYNCOPE: A CASE REPORT
Author 1 :Dr.Komaldeep
Author 2 :Dr. AP Kansal
Author 3 :Dr.Don Gregory
Author 4 : Dr.Kalpesh Patel
INTRODUCTION: Syncope is defined as a transient loss of consciousness with subsequent spontaneous recovery, resulting from global cerebral hypoperfusion. Cough syncope refers to syncope upon coughing, the pathogenesis of which is unclear and probably multi-factorial. Cough syncope is a well-recognized but uncommon phenomenon. We present a case of 34yrs male having cough as a cause for his syncope.
CASE REPORT: A 34 years-old male presented with a 2 weeks history of multiple episodes where he lost consciousness during or after cough along with jerky movements of body. The syncopal events lasted for durations ranging from 30 seconds to about one minute. All this was disturbing his routine life at home and at workplace. He was a chronic alcoholic. His weight was 97kgs and BMI was 32.4. During his hospital stay, many witnessed episodes of cough-induced syncope occurred. During the attack, his systolic blood pressure fell down to 80, his face became congested and he lost his conscious. The blood pressure returned to baseline as soon as the symptoms resolved. Symptomatic management of patient was done with cough suppressants and bronchodilators. Dietary and life style modification was advised to the patient. He was discharged a few days later for outpatient follow-up and is having no more syncopal attacks.
DISCUSSION: Cough syncope may result with serious problems such as traffic accidents, falls leading to brain and extremity injuries. Physicians should be aware of this easily recognizable cough induced syncope in all subjects admitted with syncope and should screen possible underlying sources of cough.
Author 1 :Dr.Komaldeep
Author 2 :Dr. AP Kansal
Author 3 :Dr.Don Gregory
Author 4 : Dr.Kalpesh Patel
INTRODUCTION: Syncope is defined as a transient loss of consciousness with subsequent spontaneous recovery, resulting from global cerebral hypoperfusion. Cough syncope refers to syncope upon coughing, the pathogenesis of which is unclear and probably multi-factorial. Cough syncope is a well-recognized but uncommon phenomenon. We present a case of 34yrs male having cough as a cause for his syncope.
CASE REPORT: A 34 years-old male presented with a 2 weeks history of multiple episodes where he lost consciousness during or after cough along with jerky movements of body. The syncopal events lasted for durations ranging from 30 seconds to about one minute. All this was disturbing his routine life at home and at workplace. He was a chronic alcoholic. His weight was 97kgs and BMI was 32.4. During his hospital stay, many witnessed episodes of cough-induced syncope occurred. During the attack, his systolic blood pressure fell down to 80, his face became congested and he lost his conscious. The blood pressure returned to baseline as soon as the symptoms resolved. Symptomatic management of patient was done with cough suppressants and bronchodilators. Dietary and life style modification was advised to the patient. He was discharged a few days later for outpatient follow-up and is having no more syncopal attacks.
DISCUSSION: Cough syncope may result with serious problems such as traffic accidents, falls leading to brain and extremity injuries. Physicians should be aware of this easily recognizable cough induced syncope in all subjects admitted with syncope and should screen possible underlying sources of cough.
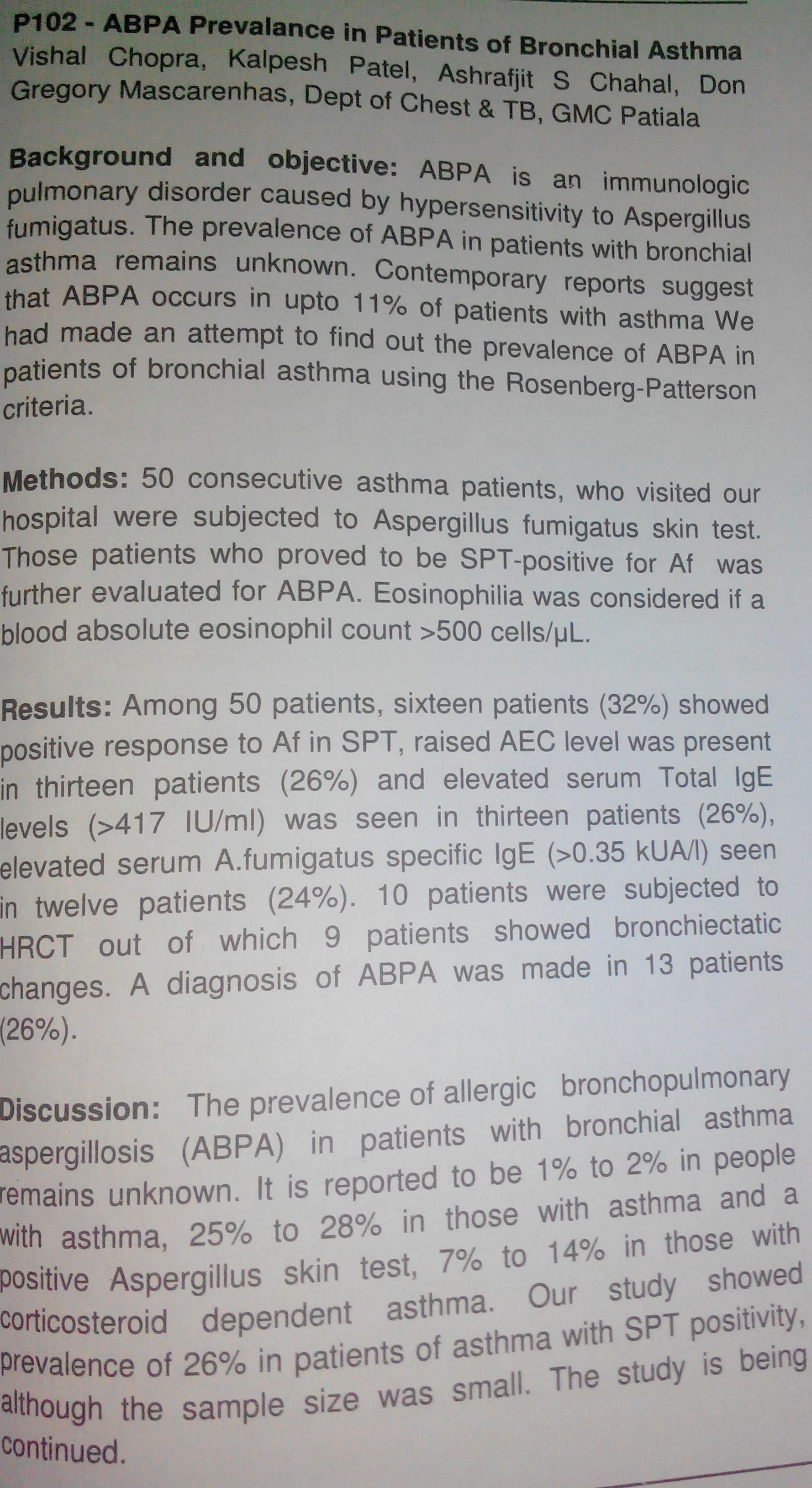
| abpa_prevalence_in_patients_of_bronchial_asthma.jpg |

{kind=link}